From 2002 to 2019, in US CENTCOM, 1,491 units of expired blood products were administered to casualties. This represented 0.4% of all blood products administered during that period.1
Is this safe, and if so, should it be part of your PACE plan for blood product use along with in-date products and dried plasma?
Researched and written by Mike Shertz, MD/18D, not AI
🕖 Reading Time, 5 minutes
The Data: Two Decades of Combat Casualty Records
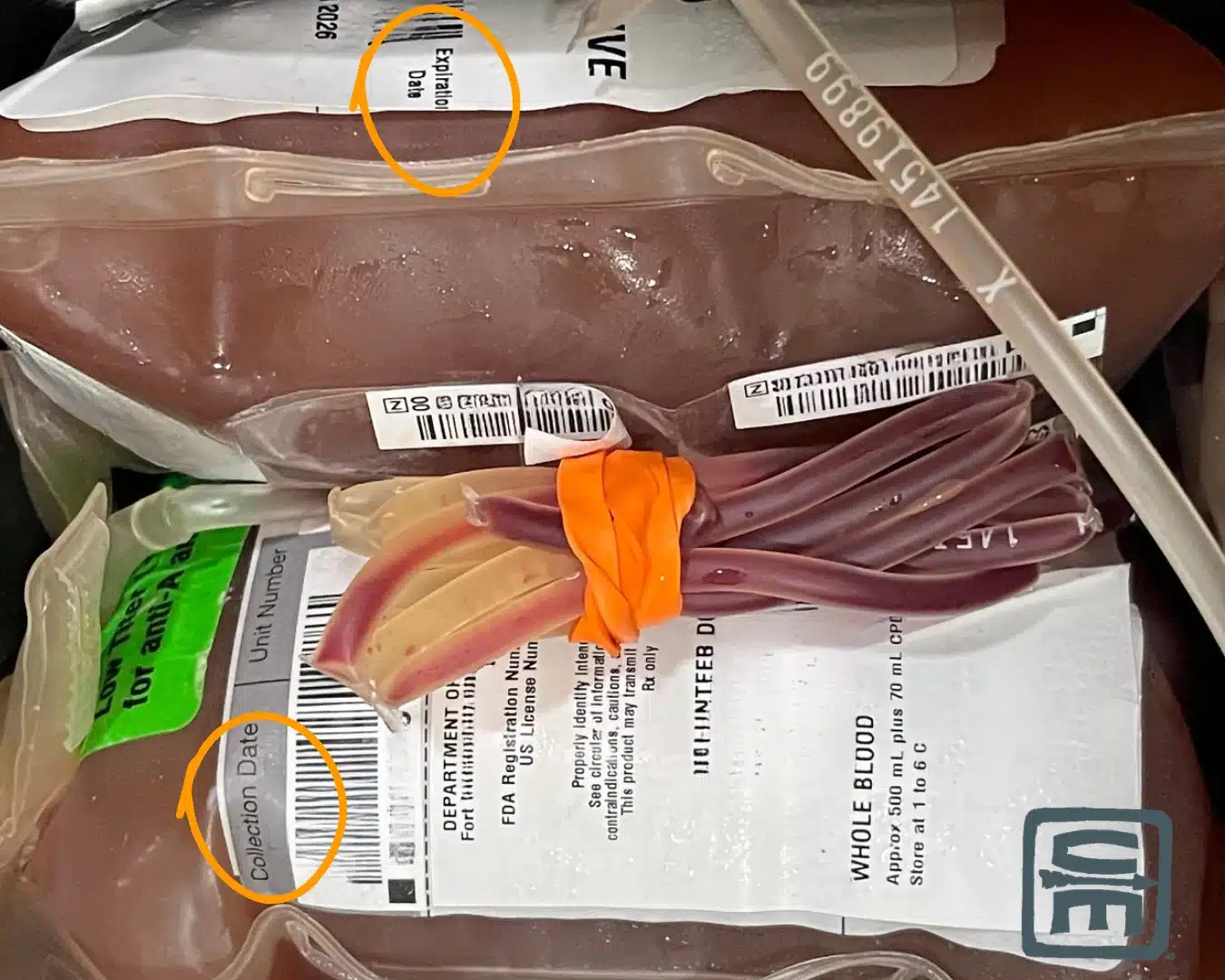
A retrospective analysis of the Armed Services Blood Program and DOD JTS records reviewed blood product transfusion over a 20-year period from Iraq, Syria, and Afghanistan looking specifically at expired products that nonetheless were still transfused.2
474 casualties received expired products. Packed RBCs were the most commonly used. One hundred patients had complete records for review, receiving 297 expired products. Of those, 86 patients received red cells and 11 whole blood. These were matched 1:4 to similar casualties receiving in date blood products.
The vast majority of red cells were only expired by 24 hours. However, some products were up to 6 days past date.2
Of the 1,491 blood products used post expiration from 2002 to 2019, 86% were no more than 3 days expired.1
Mortality Outcomes
There was no association between receiving expired products and mortality based on univariate or multivariate logistic regression. This held despite number of expired units received, presence of TBI, or amputation.2
The authors suggested “these findings were consistent with the known functional lifespan of conventional blood products which is understood to exceed regulatory shelf life.”2
Why Blood Products "Expire" in the First Place
The Association for the Advancement of Blood & Biotherapies (AABB) and the US FDA establish “blood product shelf life based on hemolysis and 24 hour recovery (how many of the transfused red cells are still in circulation at 24 hours), not clinical outcomes.”2
Specifically, an important metric is RBC hemolysis shouldn’t exceed 1% in the bag before the blood product “expires.” Hemolysis was 0.35% for whole blood and 0.21% for RBCs at the end of their storage life based on a study of six volunteer donors.3
Whole blood didn’t show any significant increase in this “storage lesion” even 21 days after expiration.3
However, another study, also of 6 volunteer collected units of whole blood, analyzed at days 35, 37, 39, and 42 showed by day 42 two of 6 units had hemolysis over 1%. The study authors noted they did remove the blood from storage and allowed it to warm every day they tested it. That is known to cause hemolysis and may have played a role in the frequency of hemolysis.4
Coagulation, Platelet Function, and Bacterial Risk
Other issues with expired blood products include impairment of coagulation potential. This was seen in both studies of volunteer collected expired whole blood. In the study of 21 day expired whole blood, this did occur, but it was no worse than packed RBCs with plasma.3
Specifically, regarding hyperkalemia in blood products, those stored 35 days did show hyperkalemia, but no further increase in potassium between day 35 and 42.4
Platelet aggregation / function was similarly impaired across both volunteer collected expired whole blood studies. Pullman, et all described this as expired whole blood basically becoming packed RBCs combined with plasma, which also has very limited platelets / platelet function. They cited civilian literature showing similar outcomes.
Despite culturing expired whole blood on days 35 and 42, no bacterial growth could be detected.4
What This Means for Your PACE Plan
If you have a hemorrhaging casualty who needs blood and all you have is appropriately stored, but slightly expired blood products (best only 24 hours old, but maybe out to 6 days) you could use them with little fear you are harming the casualty. Worst case, your whole blood became packed RBCs combined with plasma. Everything is about assets and liabilities.
Fit into a PACE plan:
Primary – unexpired whole blood
Alternate – pRBCs and some form of plasma
Contingency – recently expired whole blood (no more than 6 days, less expiration is better and more studied)
Emergency – dried plasma (has coagulation properties, but no oxygen carrying capacity)
Admittedly, you could make an argument “C” and “E” could be reversed.
References
1Lauby RS, Johnson SA, Fisher AD, April MD, Hill R, Meledeo MA, Reddoch-Cardenas KM, Bynum J, Corley J, Schauer SG. Incidence of Expired Blood Product Use in the US Central Command Theater of Operations. Med J (Ft Sam Houst Tex). 2022 Apr-Jun;(Per 22-04/05/06):40-45. PMID: 35373320.
2Riley BC, Phuong J, Hasan RA, Stansbury LG, Hess JR, Roubik DJ. Expired blood transfusion and mortality outcomes in combat trauma patients. Transfusion. 2024 Sep;64(9):1683-1691. doi: 10.1111/trf.17943. Epub 2024 Jul 5. PMID: 38965905.
3Pulliam KE, Joseph B, Veile RA, Friend LA, Makley AT, Caldwell CC, Lentsch AB, Goodman MD, Pritts TA. Expired But Not Yet Dead: Examining the Red Blood Cell Storage Lesion in Extended-Storage Whole Blood. Shock. 2021 Apr 1;55(4):526-535. doi: 10.1097/SHK.0000000000001646. PMID: 32826814; PMCID: PMC7937408.
4Greene NA, McIntosh CS, Meledeo MA, Reddoch-Cardenas KM. Hemostatic Evaluation of Refrigerated Whole Blood Stored 7 Days Post-Expiration. Mil Med. 2024 Aug 19;189(12 Suppl 3):560-567. doi: 10.1093/milmed/usae187. PMID: 38739474.