
🕖 Reading Time, 4 minutes
Typical prehospital casualty evaluation is mainly done visually with some palpation. Blood is difficult to see in lowlight settings. This has led tactical medical providers to try various strategies to care for casualties in low light and no light environments.
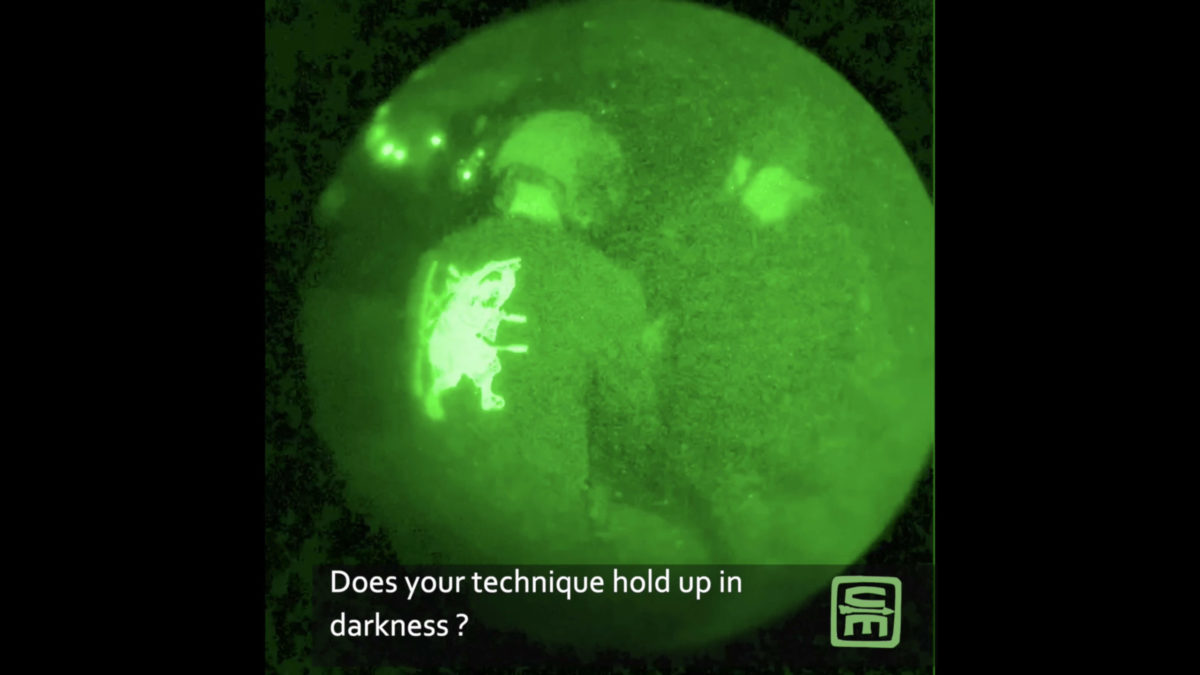
One option is to perform your casualty evaluation and life-saving interventions utilizing night vision devices. Several studies have been done testing medical procedures preformed while the provider is wearing night-vision goggles. NVGs work by amplifying ambient light or providing their infrared light.
The list of studied procedures is extensive:
- endotracheal intubation with direct and video laryngoscopy on manikins, pigs, and on humans,
- peripheral IV and IO placement,
- extremity tourniquet application
- chest tube placement
- subclavian vascular access
- cricothyroidotomy
- Jugular venous cut-down
- FAST exam with ultrasound
- laparotomy with packing
- splenectomy
- REBOA
- and thoracotomy
have all been evaluated with the provider using NODs.
[maxbutton id=”8″ ]
Multiple studies have shown that any tested procedure can be performed successfully in no light settings using NODs. Uniformly though, the procedures take longer and are more challenging.
Single chamber/tube NODs lack depth perception, and even dual chamber/tube NODs are manually focused, which makes medical procedures like intubation harder to visualize. In one study, using PVS 7s/single-tube/chamber NODs, the providers specifically had to “manually refocus the goggles as they advanced the laryngoscope blade and subsequently the endotracheal tube into the airway.”1
In a more recent study utilizing PVS 15s/dual-tube/chamber NODs surgeons “found themselves having to adjust focus multiple times throughout each procedure for optimized visualization. In order to try and overcome this, each monocle had to be set for a different focal length to be able to visualize two field depths during a procedure.” The repeated need to refocus frequently led to the breaking of aseptic technique. While not catastrophic, this is also not ideal. You will definitely contaminate your NODs with bloody hands. Additionally, the surgeons noted that due to the wavelength of the apertures, blood was partially obscured and appeared “nearly translucent” under night vision.2
Despite the published literature providing “proof of concept” that medical procedures can be successfully performed utilizing night vision devices, it is still easier, and the procedures are quicker using white light.
1Brummer S, Dickinson ET, Shofer FS, McCans JP, Mechern CC, Effect of night vision goggles on performance of advanced life support skills by emergency personnel. Mil Med. 2006 Apr;171(4):280-2.
2Derickson MJ, Kuckelman JP, Phillips CJ, et all, Life Saving Interventions in Blackout Conditions Using Night Vision Technology: Come to the Dark Side. J Trauma Acute Care Surg. 2019 Jul;87(1S Suppl 1):S191-S196.
![]()