
Best Practices: Tourniquets & Closed Femur Fractures?
Updated 18 January 2024
BLUF:* Isolated closed femur fractures are extremely rare, the internal thigh bleeding can be substantial, but tourniquet application in these closed injuries is not likely to help.
🕖 Reading Time, 4 minutes
A closed femur fracture can bleed l to 1.5 liters into the thigh musculature. This bleeding can occur from soft tissue injury from the associated sharp fracture ends, vascular injury, and bleeding from the marrow channel itself.
Periodically students ask whether there would be a role for tourniquet application on a suspected closed femur fracture if the rescuer noticed the thigh was swelling?
In a 2001 study of 4,513 civilian patients in an urban setting, only 16 presented with mid-thigh injuries. Paramedics identified five as midshaft femur fractures.1 Statistically, these are extremely rare injuries.
There is no doubt a suspected open femur fracture with massive external hemorrhage should receive tourniquet placement. However, in a suspected closed femur fracture with expanding hematoma, is there also a role for tourniquet placement?
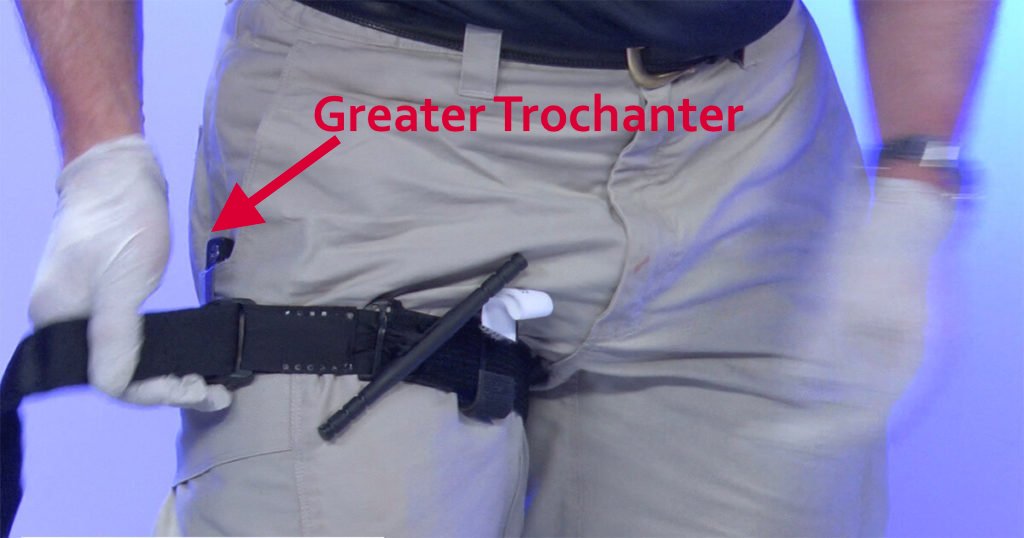
I have never seen or heard of it being done. With high and tight tourniquet application, the tourniquet would be parallel to the casualty’s perineum. In most people, that corresponds to slightly below / distal to the greater trochanter of the femur (prominent point of the femur that you can feel by pushing on your outside “hip”). Since the proximal/high femur gets its blood supply from above the greater trochanter, tourniquet placement is not likely to decrease bleeding since the tourniquet, by definition, is below where the blood supply enters the high femur. Marrow channel bleeding is likely to be unaffected by tourniquet placement since it is a rigid bony tube, and its blood supply enters proximally.
Ultimately, in a closed extremity fracture, as bleeding increases within the soft tissue, the tissue pressure will increase, which at some point will decrease the bleeding. This is basically how the iT clamp works: Trap the blood in the wound; eventually, the bleeding stops itself with its own direct pressure. Granted, in this instance, it could be 1.5 liters of blood.
One traditional argument made is that a traction splint will decrease bleeding in these fractures. The Thomas Leg Splint was designed for in-hospital femur fractures in 1875. British and French militaries fielded it during WWI. The splint supposedly saved lives in open femur fractures from gunshot wounds, though there are no studies to demonstrate this.2
IDF physicians in 2007 felt traction splints were “essential” for wartime extremity injuries. However, they noted these splints should be used for isolated femur fractures and gunshot wounds in casualties without concomitant life-threatening injuries. They also noted tourniquets specifically should not be used for femur fractures, citing likely failure and potential further injury. We presume they are referring to femur fractures without significant external bleeding. We would absolutely place a tourniquet for a femoral artery bleed associated with an open femur fracture.2
Life in the Fastlane3 did a nice literature review of traction splints. Their conclusion? There have only been five studies cumulatively providing very little evidence. The studies show traction splints are often applied to casualties with contraindications to the application, take up a lot of space, and have minimal evidence of benefit. Even the IDF acknowledges a traction splint may not be needed in urban settings, noting that simply tying the casualty’s legs together may suffice for adequate fracture mobilization.
A systematic review on traction splints published in 2023 showed all fracture splinting decreases pain, but without clear benefit, a traction splint does it better for a femur fracture than regular splinting. They cited literature indicating there might be a reduced need for blood products in a femur fracture if a traction splint is applied. The agree there is no other evidence of benefit using a traction splint.4
Interested to learn more? Try our online courses, or get started with a sample of the material in the preview course
Preview CourseNot sure? Try a preview TRAIN NOWOnline Tactical Casualty Care Classes
References:
*For those unfamiliar with this term, BLUF is “Bottom Line Up Front,”
1Abarbanell NR. Prehospital midthigh trauma and traction splint use: recommendations for treatment protocols. Am J Emerg Med. 2001 Mar;19(2):137-40.
2Sacred Cow Slaughterhouse: The Traction Splint. https://www.emsworld.com/article/11542786/sacred-cow-slaughterhouse-traction-splint
3Femoral traction splints, helpful or not https://litfl.com/femoral-traction-splints-helpful-or-not/
4Philipsen SPJ, Vergunst AA, Tan ECTH. Traction Splinting for midshaft femoral fractures in the pre-hospital and Emergency Department environment – A systematic review. Injury. 2022 Dec;53(12):4129-4138.



{kind=link}