Shock Index: a more sophisticated determinant of hypovolemic shock
Although not as convenient as evaluating the “Go / No Go” presence of a casualty’s radial pulse, their “shock index” is a much more sophisticated snapshot of their hypovolemic status. Shock index is a ratio of the trauma patient’s heart rate divided by their systolic blood pressure.Simply put, anytime a casualty’s heart rate is higher than their systolic blood pressure, that’s bad.
Initially proposed in 1967, the shock index has recently gained favor as a more reliable predictor of hypovolemia in trauma patients than the heart rate or blood pressure alone.
In concept, as a patient loses blood, their heart rate should increase to circulate the remaining volume faster. In trauma patients with systolic blood pressures less than 90 mmHg, only 71% also have heart rates over 100 beats per minute.1 Unfortunately, that means despite being hypotensive, nearly 1/3 of trauma patients have normal heart rates. This isn’t just a byproduct of the prevalence of antihypertensive medications but is just how some patients respond to hypovolemia.
Interestingly, when healthy volunteers donate 450 ml of blood, their heart rate and systolic blood pressure remains in the normal range after donation; however, their shock index increases.
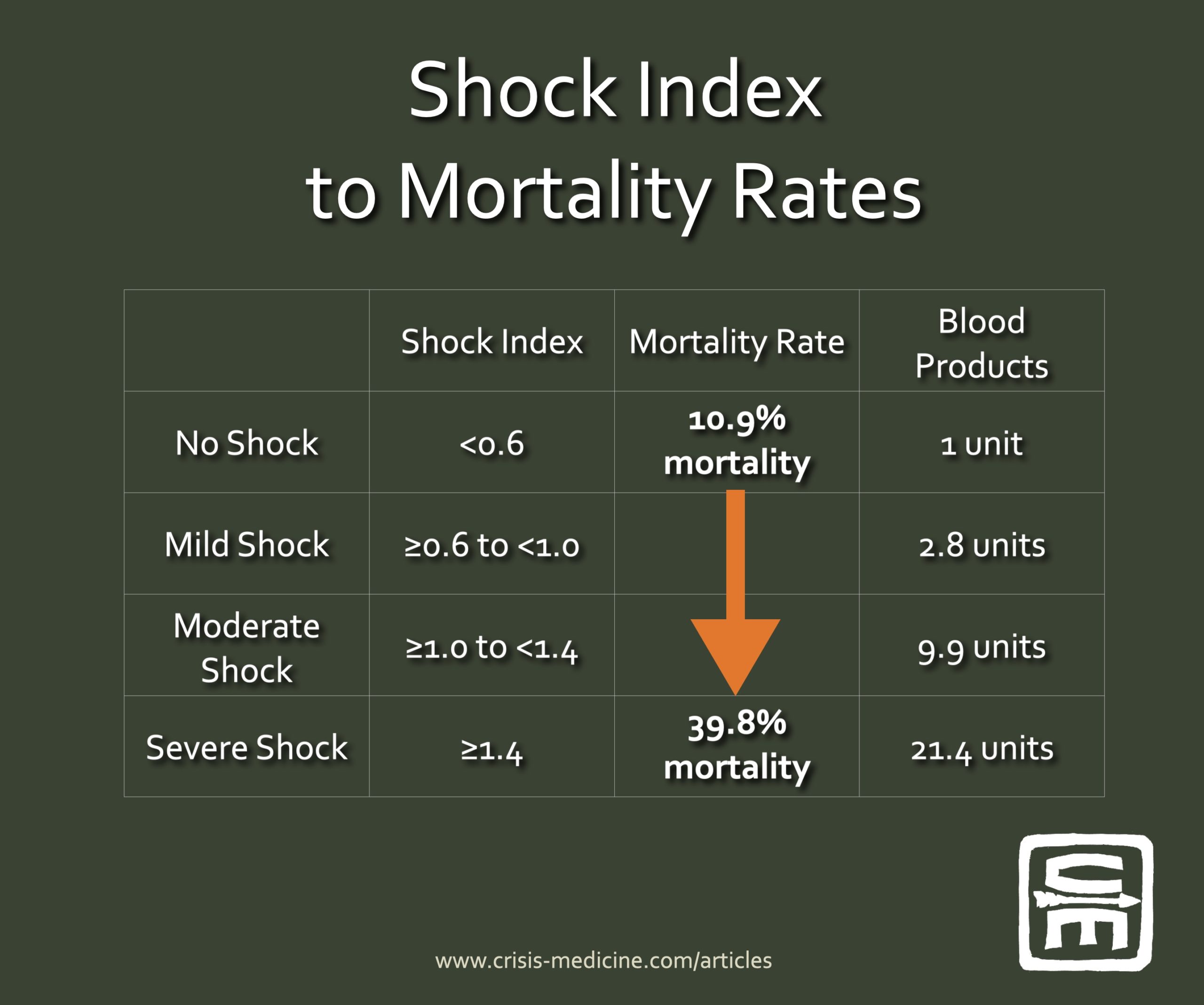
Shock index (SI) is broken into four groups:
no shock is a SI of <0.6,
mild shock ≥0.6 to <1.0,
moderate shock ≥1.0 to <1.4,
and severe shock ≥1.4.
Applying this concept to 21,853 trauma patients in a German registry showed that as a patient’s shock index increases, they have a corresponding increase in mortality, trauma-induced coagulopathy, transfusion requirement, the likelihood of massive transfusion (more than ten units of blood in the first 24 hours), and higher rates of intubation.2 The patients with a normal shock index (<0.6) had a 10.9% mortality and received on average one unit of blood. In the group with severe shock (≥1.4), the mortality rate increased to 39.8% and received an average of 21.4 units of blood.
Casualties with a SI of ≥1.4 are twenty-times more likely to receive a massive transfusion. There is also a fivefold increase in mortality if the casualty’s SI increases ≥0.3 between prehospital and ED readings.
Though most studied in trauma patients, literature showing the shock index is also valid in gastrointestinal bleeds and ruptured ectopic pregnancies.
Because children have higher heart rates and lower systolic blood pressures at baseline, the shock index can’t be used as-is for pediatrics. There are a few studies applying an adjusted version to pediatric trauma, but as significant pediatric trauma is unusual and largely blunt trauma, this literature is evolving.