MIST Report: A simple way to convey information
- Posted by Mike Shertz MD/18D
- Categories MARCH, More
Within EMS there is great inconsistency as to what information is conveyed to the next level of medical provider.
🕖 Reading Time, 3 minutes
In a qualitative analysis of 90 EMS to Emergency Department handoffs of critically ill patients, the chief concern or complaint was provided only 78% of the time. Only half of the handoffs included pertinent physical exam findings.1 Much of this stems from a lack of consistent expectation as to what information the ED wants from EMS. Additionally, only about half of the information conveyed verbally between EMS and the ED is retained by the ED personnel following the verbal transfer.2
To fix this problem, EMS systems need to engage the ED’s they interact with to establish consistent expectations for the patient hand-off process and determine what information is useful and desired. Since very little of the verbal report is actually remembered, giving a more concise report would be helpful to identify the critical information.
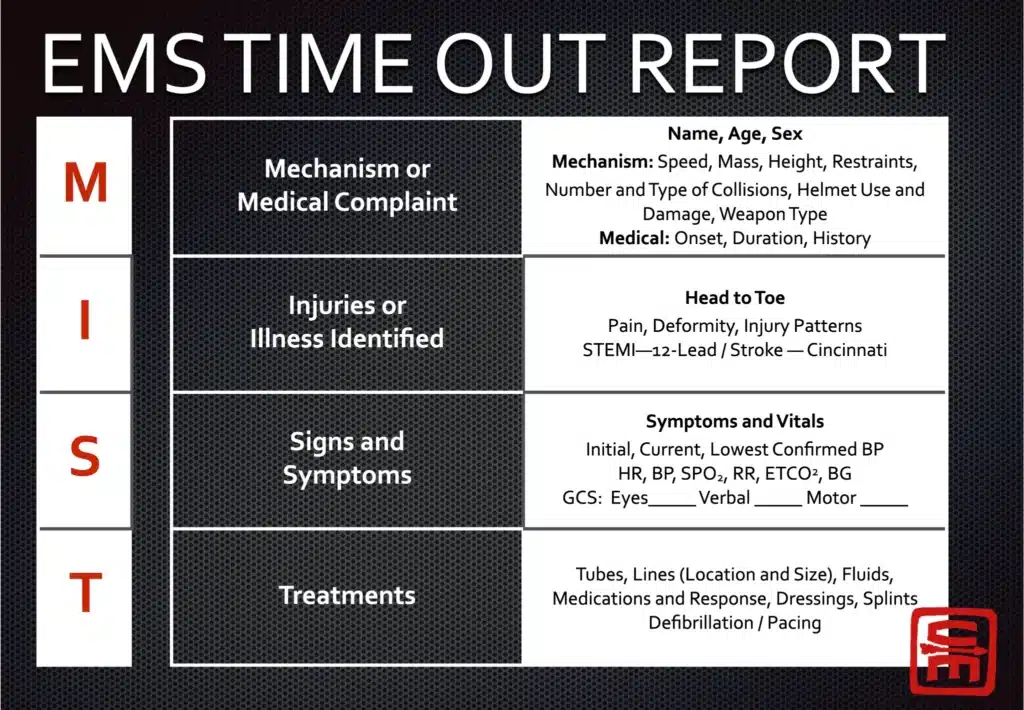
For all levels of medical providers, a very simple verbal report format is the MIST report used by the military. Although it may not convey all the detailed information regarding allergies and medications sometimes included in a more traditional EMS report, it gets to the salient details rapidly.
M – Mechanism
A simple description of the mechanism of injury, i.e., gunshot wound, explosion, fire, building collapse, etc.
I – Injuries
Often combined with the mechanism, i.e., gunshot wound to the leg, bilateral leg amputations from an explosion, severe maxillofacial injury, etc.
S – Signs / Symptoms
Massive hemorrhage, not following commands, no radial pulse, abnormal respiratory rate, oxygen saturation if abnormal, struggling to breathe, audible stridor, etc.
T -Treatment
What was done for the casualty to fix the above-noted issues? i.e., side-by-side tourniquets, wound packed, surgical airway placed, needle decompression for presumed tension pneumothorax, etc.
An example of a MIST report might be: “This is an adult male with a gunshot wound the thigh, massive hemorrhage controlled with two side by side tourniquets, he doesn’t follow commands, and has no radial pulse. His carotid pulse is 130. ”
For the first several minutes of resuscitation and evaluation, the next higher medical providers know everything they need to. This casualty is in shock, hypotensive, but no longer bleeding. He needs fluid resuscitation, preferably with blood. The exact timing of his last meal is unimportant as he is going to surgery regardless.
Another example: “This is an adult male police officer with a gunshot wound to the neck, expanding hematoma, massive hemorrhage, and stridor. He doesn’t follow commands and has no radial pulse. His would is packed, and a surgical airway was placed. His stridor resolved, and he is breathing 30 breaths a minute.”
Again, we know what we need to for immediate treatment. The patient has a penetrating neck injury with likely vascular injury and airway obstruction. He is in shock, but currently a satisfactory airway.
Finally, a third example: “This is an adult male with a gunshot wound to the chest. He had no radial pulse and was struggling to breathe. He had minimal external bleeding. He underwent needle decompression with return of his radial pulse and decreased work of breathing.”
This simple, focused verbal report can help the next provider concentrate on the major issues first. They can figure out medications and allergies once all life threats have been dealt with. Certainly, this model could be expanded to include all patient handoffs and many EMS systems have done just that.
Interested in learning how to stop massive hemorrhage and be an immediate responder in an emergency? Try our online courses, or get started with a sample of the material in the preview course
Preview CourseNot sure? Try a preview TRAIN NOWOnline Tactical Casualty Care Classes
1Goldberg, S. A., Porat, A. (2017). Quantitative analysis of the content of EMS handoff of critically ill and injured patients to the emergency department. Prehospital Emergency Care, 21(1), 14-17.
2Talbot, R., & Bleetman, A. (2007). Retention of information by emergency department staff at ambulance handover: do standardized approaches work?. Emergency Medicine Journal, 24(8), 539-542.
Dr. Mike Shertz is the Owner and Lead Instructor at Crisis Medicine. Dr. Shertz is a dual-boarded Emergency Medicine and EMS physician, having spent over 30 years gaining the experience and insight to create and provide his comprehensive, science-informed, training to better prepare everyday citizens, law enforcement, EMS, and the military to manage casualties and wounded in high-risk environments. Drawing on his prior experience as an Army Special Forces medic (18D), two decades as an armed, embedded tactical medic on a regional SWAT team, and as a Fire Service and EMS medical director.
Using a combination of current and historical events, Dr. Shertz’s lectures include relevant, illustrative photos, as well as hands-on demonstrations to demystify the how, why, when to use each emergency medical procedure you need to become a Force Multiplier for Good.