🕖 Reading Time, 4 minutes
Reviews of most mass casualty events have shown that rarely is a preplanned triage system actually used in the event. Triage is a French word for sorting. Although there are many systems to help first responders triage casualties into categories of those who need treatment now versus those who can wait, it is very challenging to use most of those systems in chaotic and dangerous environments like mass casualty events.
Even systems that appear simple and require the evaluation of only a handful of variables quickly become overwhelming when multiple people require immediate medical care under the continually evolving situations of active violent incidents and natural disasters.
Reviews of most mass casualty events have shown that rarely is a preplanned system actually used in the event.
If you don’t have a way to sort casualties, resources might be devoted to injured that don’t really need them, while “sicker” patients go unrecognized and untreated and do not receive the proper medical care in the time they need it.
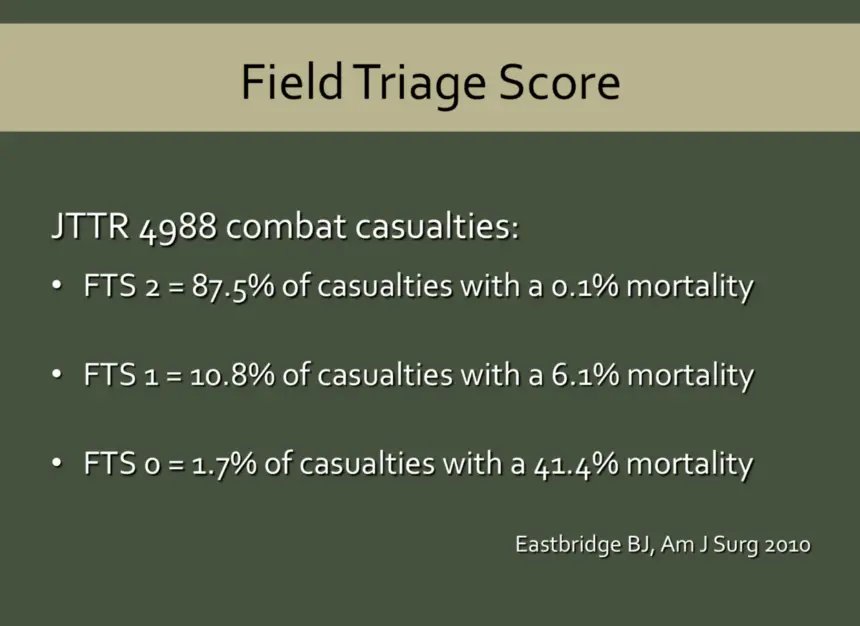
The Field Triage Score is a simple technique to sort casualties in frenzied and tumultuous environments. 1
Military authors evaluated 4,988 casualties from the war in Iraq and Afghanistan. They looked at two factors: The casualty’s ability to follow a command (a normal GCS motor score) and whether the casualty’s blood pressure was over 100 mm Hg. They then divided the casualties into three groups by those variables. One group was able to follow a simple command and had a BP above 100 mm Hg. One group couldn’t follow a simple command and did not have a BP above 100 mmHg. The final group had one or the other, but not both.
Using those three categories the authors looked at the length of hospitalization (a marker of how sick the casualties were) and the casualty’s mortality (death rate).
The authors sought to make this triage system more useful and easier to apply in chaotic and dangerous prehospital environments. Therefore, they suggested relying on the presence of a normal radial pulse instead of an actual blood pressure value. There is medical literature to support the concept.2
The value of this simple triage system is the black-or-white, go-or-no-go quality of the data points.
You can either follow a simple command, (show me two fingers, point to where you are hurt, squeeze my hand) or you can’t. No partial credit is given. As for the radial pulse: It either feels normal or not. Simple. Black and white.
With this simple technique, minimally trained individuals can quickly sort casualties into the sickest, somewhat-sick, and not-sick categories very easily. This frees higher medical care providers time to provide more care in the critical aftermath of an event.
 Imagine a Casualty Collection Point where as each new casualty arrives someone checks their ability to follow a command and for the presence of a radial pulse.
Imagine a Casualty Collection Point where as each new casualty arrives someone checks their ability to follow a command and for the presence of a radial pulse.
With this simple technique, first responders can quickly and efficiently triage casualties.
One critique of this technique is that it was retrospectively created by looking at the casualty’s blood pressure and ability to follow commands on arrival to a medical treatment facility. It has not been prospectively evaluated in a prehospital environment. However, since almost all actual events fail to use triage systems, it seems a more straightforward and reasonable option to evaluate casualties and ensure the sickest patients are quickly provided life-saving interventions.
Footnotes:
1Eastridge BJ, Butler F, Wade C, et al. Filed triage score (FTS) in battlefield casualties: validation of a novel triage technique in a combat environment. Am J Surg 2010;200(6):724-7. https://www.ncbi.nlm.nih.gov/pubmed/21146011
2McManus J, Yershov AL, Ludwig D, et al. Radial pulse character relationship to systolic blood pressure and trauma outcomes. Prehosp Emerg Care 2005;9:423-8. https://www.ncbi.nlm.nih.gov/pubmed/21146011