Showing 1-6 of 66 results
MARCH: Massive Hemorrhage, Airway, Respiration, Circulation, Hypothermia Prevention
The easy to remember mnemonic MARCH reminds us of the priorities in treating casualties during TECC and TCCC situations. MARCH provides a framework to address immediate life threats and gives an organized approach to begin a casualty evaluation. The MARCH mnemonic is preferable to the ABCDE model because it takes into consideration the reason you need an airway and to be breathing is to circulate blood to the casualty’s brain. Recognizing that, the first step in our casualty evaluation should be to look for massive hemorrhage.
Once past massive hemorrhage, A-R-C is loosely approximated by A-B-C. H- is a reminder that a large number of traumatic casualties arrive at the emergency department or medical treatment facility hypothermic which dramatically increases their death rate.
The MARCH mnemonic can be applied to any patient, as the initial casualty evaluation usually rules out massive hemorrhage.
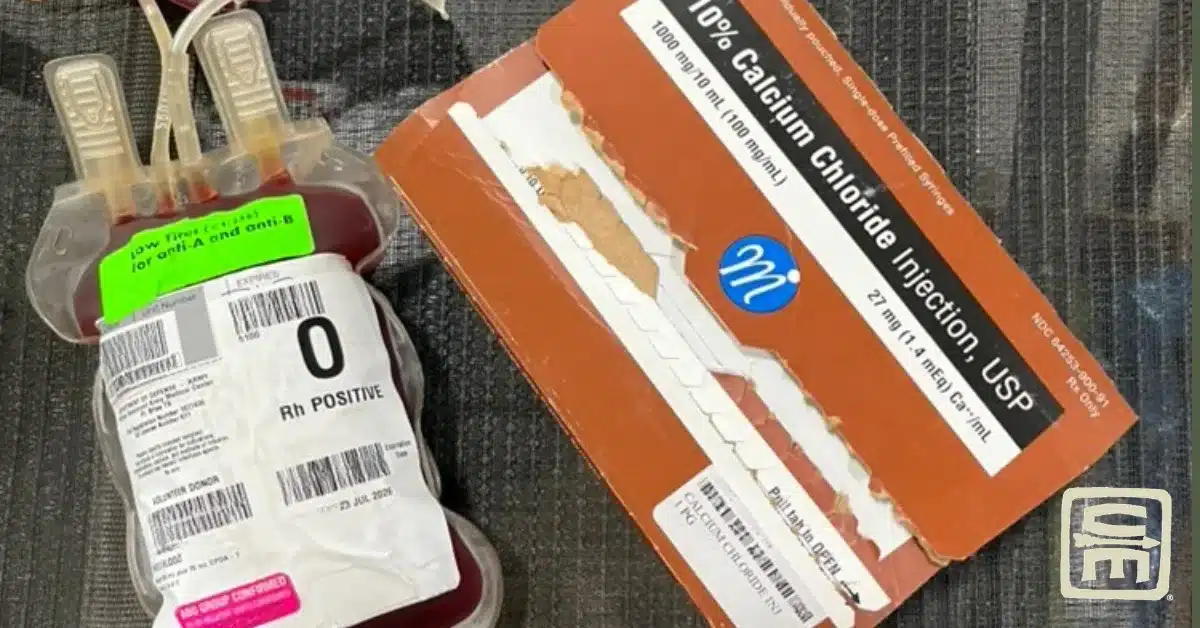
Recently there has been an increase in discussions regarding hypercalcemia and trauma patients. Preliminary evidence suggests being traumatically injured and having an abnormally high calcium level is just as detrimental as hypocalcemia. 🕖 Reading Time, 4 minutes Researched and written …
From 2002 to 2019, in US CENTCOM, 1,491 units of expired blood products were administered to casualties. This represented 0.4% of all blood products administered during that period.1 Is this safe, and if so, should it be part of your …
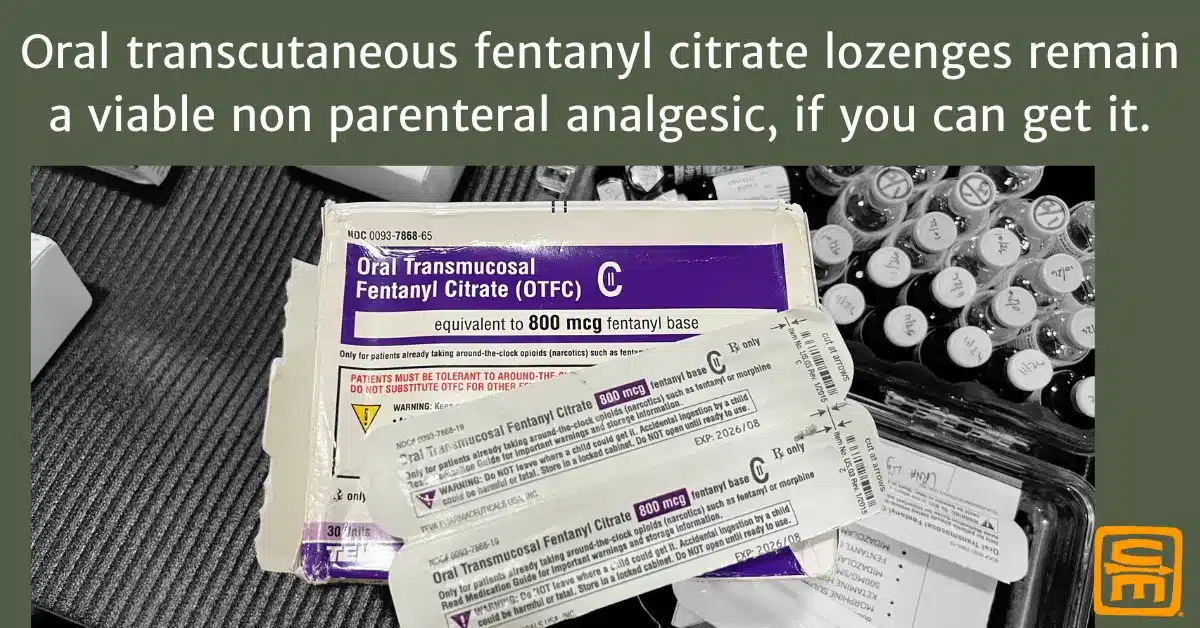
🕖 Reading Time, 4 minutes Researched and written by Mike Shertz, MD/18D, not AI Oral transmucosal fentanyl citrate (OTFC) was recently removed from the TCCC guidelines. It wasn’t removed because new literature showed it doesn’t work or causes complications. It …
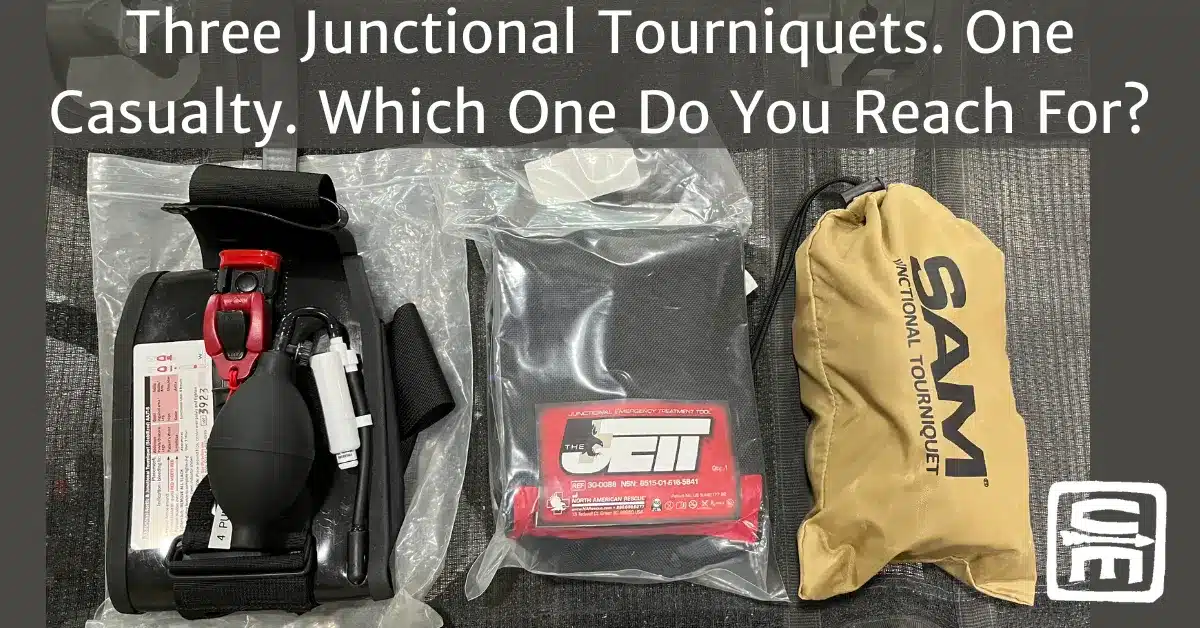
Three Junctional Tourniquets. One Casualty. Which One Do You Reach For? Researched and written by Mike Shertz, MD/18D, not AI 🕖 Reading Time, 2 minutes Miyamoto Musashi one of Japan’s most famous samurai and author of “the book of five …
There is a new JTS CPG for freeze dried plasma use, updated 09 June 2026. Researched and written by Mike Shertz, MD/18D, not AI 🕖 Reading Time, 2 minutes One such product, OctaplasLG is a freeze dried plasma approved by …
Researched and written by Mike Shertz, MD/18D, not AI 🕖 Reading Time, 4 minutes Creatively free-thinking under stress is extremely difficult. Learn to see improvised techniques in your every day environment and they will occur to you when you need …