1Yost J, Baldwin P, Bellenger S, Bradshaw F, Causapin E, Demotica R, Livingston M, Lee C, Gegel B, Burgert J, Claessens A, Johnson D, Loughren M. The pharmacokinetics of intraosseous atropine in hypovolemic swine. Am J Disaster Med. 2015 Autumn;10(3):217-22.
2Eisenkraft A, Gilat E, Chapman S, Baranes S, Egoz I, Levy A. Efficacy of the bone injection gun in the treatment of organophosphate poisoning. Biopharm Drug Dispos. 2007 Apr;28(3):145-50.
3Krueger GP. Psychological and performance effects of chemical-biological protective clothing and equipment. Mil Med. 2001 Dec;166(12 Suppl):41-3.
4Castle N, Owen R, Hann M, Clark S, Reeves D, Gurney I. Impact of chemical, biological, radiation, and nuclear personal protective equipment on the performance of low- and high-dexterity airway and vascular access skills. Resuscitation. 2009 Nov;80(11):1290-5.
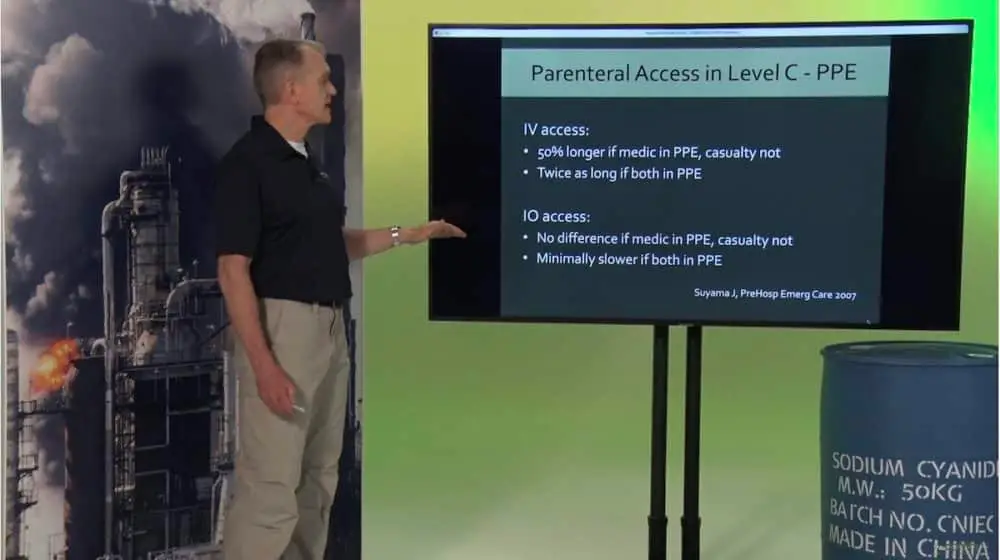
5Suyama J, Knutsen CC, Northington WE, Hahn M, Hostler D. IO versus IV access while wearing personal protective equipment in a HazMat scenario. Prehosp Emerg Care. 2007 Oct-Dec;11(4):467-72.
6Mormando G, Paganini M, Alexopoulos C, Savino S, Bortoli N, Pomiato D, Graziano A, Navalesi P, Fabris F. Life-Saving Procedures Performed While Wearing CBRNe Personal Protective Equipment: A Mannequin Randomized Trial. Simul Healthc. 2021 Dec 1;16(6):e200-e205.